È un tipo di tumore molto raro (<1% di tutte le neoplasie mammarie) e aggressivo di carcinoma invasivo della mammella, caratterizzato da punteggio Ki-67 elevato (elevata aggressività e crescita rapida) e dimensioni relativamente grandi, con tendenza alla metastizzazione, in particolare ai polmoni, ossa e cervello, e interessamento relativamente meno frequente dei linfonodi del cavo ascellare.
Dal punto di vista istologico, il tumore presenta cellularità di grado elevato e differenziazione eterologa (da cui la denominazione metastatica), con elementi condroidi, ossei, pleomorfi/sarcomatoidi, fusiformi e squamosi. 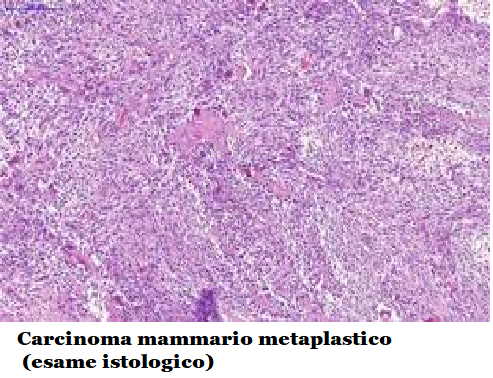
Diagnosi: di solito è presente una massa di grosse dimensioni, mobile, ben circoscritta; la massa cresce rapidamente, può essere dolorosa e interessare la parete toracica e la cute, causando ulcerazioni.
Esami strumentali: mammografia, ecografia, aspirazione con ago sottile (FNA), biopsia centrale.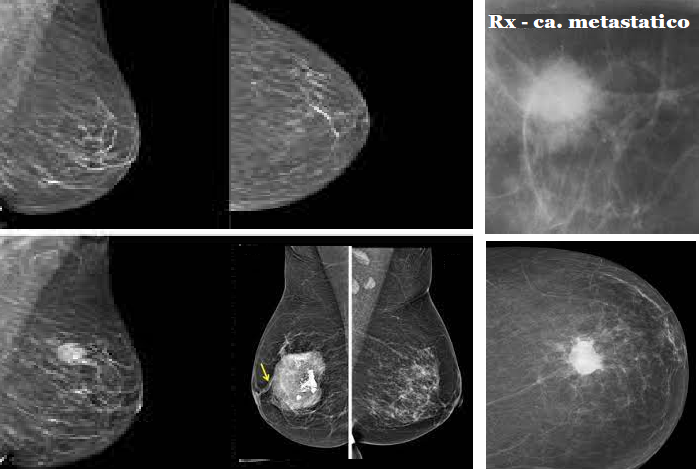
L’esame USG fornirà ulteriori elementi su morfologia ed estensione del carcinoma.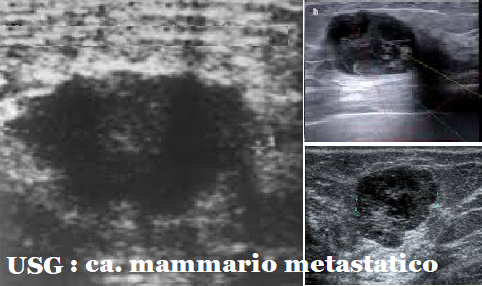
Terapia: il trattamento locale (chirurgia e radioterapia) sono in linea generale uguali agli altri tipi di tumore.
I tumori metaplastici all’esame istologico presentano abitualmente un fenotipo triplo negativi e e frequentemente mutazioni di TP53. Nei carcinomi metaplastici non è perciò indicata né una terapia ormonale né la terapia biologica mirata (terapia a bersaglio) con Trastuzumab (Herceptin®).
La chemioterapia rappresenta perciò il trattamento precauzionale di scelta in questi tumori. I farmaci chemioterapici più utilizzati sono:
- antracicline: doxorubicina (Adriamycin) o l’epirubicina (Ellence)
- taxani: paclitaxel (Taxol) o docetaxel (Taxotere).
Sei cicli di questa chemioterapia da quattro a sei mesi prima dell’intervento chirurgico che prevede mastectomia totale, lumpectomia ed eventuale linfadenectomia ascellare in caso di positività del linfonodo sentinella.
È importante sottolineare che esistono due sottotipi di carcinoma metaplastico che presentano bassi livelli di aggressività, ovvero il carcinoma tipo-fibromatoso e il carcinoma adenosquamoso di basso grado. Da un punto di vista istologico i carcinomi fibromatosis-like a cellule fusate devono essere distinti dalla fibromatosi desmoide e altre forme benigne a cellule fusate della mammella, che seppure siano meno aggressivi dei carcinomi metaplastici, hanno tuttavia a lungo termine un potenziale metastatico e devono essere trattati chirurgicamente come carcinomi.
References:
- A brief overview of the WHO classification of breast tumors, 4th edition, focusing on issues and updates from the 3rd edition. Sinn HP, Kreipe H. Breast Care (Basel) 2013;8:149–154.
- Management and outcomes in metaplastic breast cancer. Tzanninis IG, Kotteas EA, Ntanasis-Stathopoulos I, Kontogianni P, Fotopoulos G. Clin Breast Cancer. 2016;16:437–443.
- Metaplastic breast cancer: clinical overview and molecular aberrations for potential targeted therapy. Abouharb S, Moulder S. Curr Oncol Rep. 2015;17:431.
- The prognostic significance of metaplastic carcinoma of the breast (MCB)–a case controlled comparison study with infiltrating ductal carcinoma. Lai HW, Tseng LM, Chang TW, et al. Breast. 2013;22:968–973.
- Unique clinicopathological features of metaplastic breast carcinoma compared with invasive ductal carcinoma and poor prognostic indicators. Song Y, Liu X, Zhang G, et al. World J Surg Oncol. 2013;11:129.
- Characteristics and treatment of metaplastic breast cancer: analysis of 892 cases from the National Cancer Data Base. Pezzi CM, Patel-Parekh L, Cole K, Franko J, Klimberg VS, Bland K. Ann Surg Oncol. 2007;14:166–173.
- Lakhani SR, Ellis IO, Schnitt SJ, Tan PH, van de Vijver MJ. Lyon, France: World Health Organization; 2012. WHO classification of tumours of the breast who classification of tumours, 4th edition, volume 4.
- Prognostic factors in metaplastic carcinoma of the breast: a multi-institutional study. Rakha EA, Tan PH, Varga Z, et al. Br J Cancer. 2015;112:283–289.
- Metaplastic breast cancer: histologic characteristics, prognostic factors and systemic treatment strategies. Schwartz TL, Mogal H, Papageorgiou C, Veerapong J, Hsueh EC. Exp Hematol Oncol. 2013;2:31.
- 10. Clinicopathological features and prognosis of metaplastic breast carcinoma: experience of a major Chinese Cancer Center. Zhang Y, Lv F, Yang Y, et al. PLoS One. 2015;10:0. [PMC free article] [PubMed] [Google Scholar]
- Genomic profiling of metaplastic breast carcinomas reveals genetic heterogeneity and relationship to ductal carcinoma. Krings G, Chen YY. Mod Pathol. 2018;31:1661–1674.
- Genomic and transcriptomic heterogeneity in metaplastic carcinomas of the breast. Piscuoglio S, Ng CK, Geyer FC, et al. NPJ Breast Cancer. 2017;3:48.
- p63 is useful in the diagnosis of mammary metaplastic carcinomas. Tse GM, Tan PH, Chaiwun B, et al. Pathology. 2006;38:16–20.
- Diagnostic utility of snail in metaplastic breast carcinoma. Nassar A, Sookhan N, Santisteban M, Bryant SC, Boughey JC, Giorgadze T, Degnim A. Diagn Pathol. 2010;5:76.
- Metaplastic carcinoma of the breast. McKinnon E, Xiao P. Arch Pathol Lab Med. 2015;139:819–822.
- Metaplastic carcinoma of the breast: a clinicopathological review. Tse GM, Tan PH, Putti TC, Lui PC, Chaiwun B, Law BK. J Clin Pathol. 2006;59:1079–1083.
- Predictive factors on outcomes in metaplastic breast cancer. Leyrer CM, Berriochoa CA, Agrawal S, et al. Breast Cancer Res Treat. 2017;165:499–504.
- The prognoses of metaplastic breast cancer patients compared to those of triple-negative breast cancer patients. Bae SY, Lee SK, Koo MY, et al. Breast Cancer Res Treat. 2011;126:471–478.
- Metaplastic carcinoma of the breast, an unusual disease with worse prognosis: the experience of the European Institute of Oncology and review of the literature. Luini A, Aguilar M, Gatti G, et al. Breast Cancer Res Treat. 2007;101:349–353.
- Metaplastic breast cancer: a comparison between the most common histologies with poor immunohistochemistry factors. Barquet-Muñoz SA, Villarreal-Colin SP, Herrera-Montalvo LA, et al. BMC Cancer. 2015;15:75.
- Survival outcomes of metaplastic breast cancer patients: results from a US population-based analysis. Nelson RA, Guye ML, Luu T, Lai LL. Ann Surg Oncol. 2015;22:24–31.
- Metaplastic carcinoma of the breast is more aggressive than triple-negative breast cancer: a study from a single institution and review of literature. El Zein D, Hughes M, Kumar S, Peng X, Oyasiji T, Jabbour H, Khoury T. Clin Breast Cancer. 2017;17:382–391.
- Biphasic metaplastic sarcomatoid carcinoma of the breast. Hennessy BT, Giordano S, Broglio K, et al. Ann Oncol. 2006;17:605–613.
- Metaplastic breast cancer: clinical significance. Beatty JD, Atwood M, Tickman R, Reiner M. Am J Surg. 2006;191:657–664.
- Metaplastic carcinomas of the breast. I. Matrix-producing carcinoma. Wargotz ES, Norris HJ. Hum Pathol. 1989;20:628–635.
- 26. Worse prognosis of metaplastic breast cancer patients than other patients with triple-negative breast cancer. Jung SY, Kim HY, Nam BH, et al. Breast Cancer Res Treat. 2010;120:627–637.
- 27. Metaplastic breast cancer: clinicopathological features and its prognosis. Lee H, Jung SY, Ro JY, et al. J Clin Pathol. 2012;65:441–446.
- Metaplastic breast carcinoma: a clinical analysis of 26 cases. Jin X, Yu D, Guo C, Gong X, Li N, Zhao Y. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6958196/ Int J Clin Exp Pathol. 2018;11:2112–2117.
- Metaplastic breast carcinoma: analysis of 31 cases from a single institute. Fayaz S, Demian GA, Eissa HE, Amanguno H, Abuzalouf S. J Egypt Natl Canc Inst. 2017;29:141–145.
- Metaplastic sarcomatoid carcinoma of the breast appears more aggressive than other triple receptor-negative breast cancers. Lester TR, Hunt KK, Nayeemuddin KM, et al. Breast Cancer Res Treat. 2012;131:41–48.